Abstract
Introduction: Hypertriglyceridemia is a known cause of electrolyte derangements. Though the mechanism is not fully understood, it is presumed to be due to light scattering effects during spectrophotometry. A high index of suspicion in the context of clinical picture is important to avoid unnecessary testing.
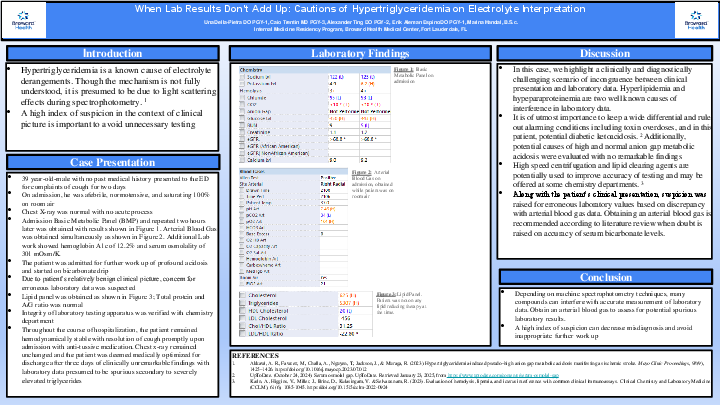
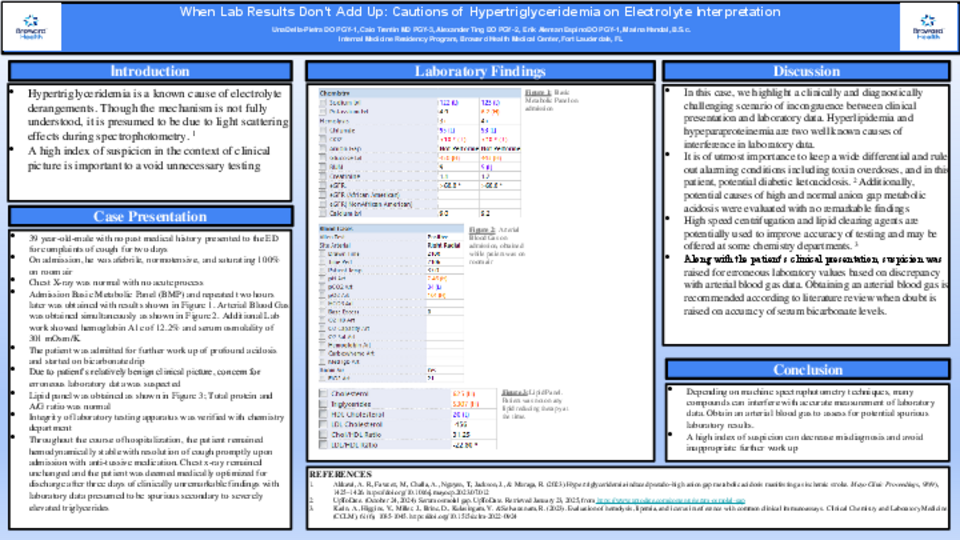
Case Presentation: A 39 year-old-male with no past medical history presented to the ED for complaints of cough for two days. On admission, he was afebrile, normotensive, and saturating 100% on room air. Chest X-ray was normal with no acute process. Admission Basic Metabolic Panel (BMP) and repeated two hours later and showed a severe metabolic acidosis, hyponatremia, and hypochloremia. Arterial Blood Gas was obtained and showed an incongruent mild respiratory alkalosis metabolic with secondary metabolic acidosis. Additional Lab work showed hemoglobin A1c of 12.2% and serum osmolality of 301 mOsm/K. The patient was admitted for further work up of profound acidosis and started on bicarbonate drip. Due to patient’s relatively benign clinical picture, concern for erroneous laboratory data was suspected. Lipid panel was obtained with triglycerides found to be 5307; Total protein and A/G ratio was normal. Integrity of laboratory testing apparatus was verified with chemistry department. Throughout the course of hospitalization, the patient remained hemodynamically stable with resolution of cough promptly upon admission with anti-tussive medication. Chest x-ray remained unchanged and the patient was deemed medically optimized for discharge after three days of clinically unremarkable findings with laboratory data presumed to be spurious secondary to severely elevated triglycerides.
Discussion: In this case, we highlight a clinically and diagnostically challenging scenario of incongruence between clinical presentation and laboratory data It is of utmost importance to keep a wide differential and rule out alarming conditions including toxin overdoses, and in this patient, potential diabetic ketoacidosis. Additionally, potential causes of high and normal anion gap metabolic acidosis were evaluated with no remarkable findings. Along with the patient’s clinical presentation, suspicion was raised for erroneous laboratory values based on interpretation with the arterial blood gas.High speed centrifugation and lipid clearing agents are potentially used to improve accuracy of testing and may be offered at some chemistry departments.
Conclusion: Depending on machine spectrophotometry techniques, many compounds can interfere with accurate measurement of laboratory data. Obtain an arterial blood gas to assess for potential spurious laboratory results. A high index of suspicion can decrease misdiagnosis and avoid inappropriate further work up.